
General examination
A thorough examination is important in these patients since many rheumatologic disorders are multi-systemic in nature. The patient should be undressed and covered with an examination gown. The musculoskeletal examination can be integrated into the general examination, as is done by subspecialists , or performed, as a separate unit. Regardless, movement of the patient should be kept to a minimum because of associated pain and difficulty.
Recommended sequence:
Seated on the examination table:
- Hands
- Wrists
- Elbows
- Shoulders
- Neck and upper back
Laying down on the examination table:
- Hips
- Knees
- Ankles
- Feet
Standing:
- Popliteal regions
- Calves
- Arches of the Feet
- Lower back movement
- Stance and gait
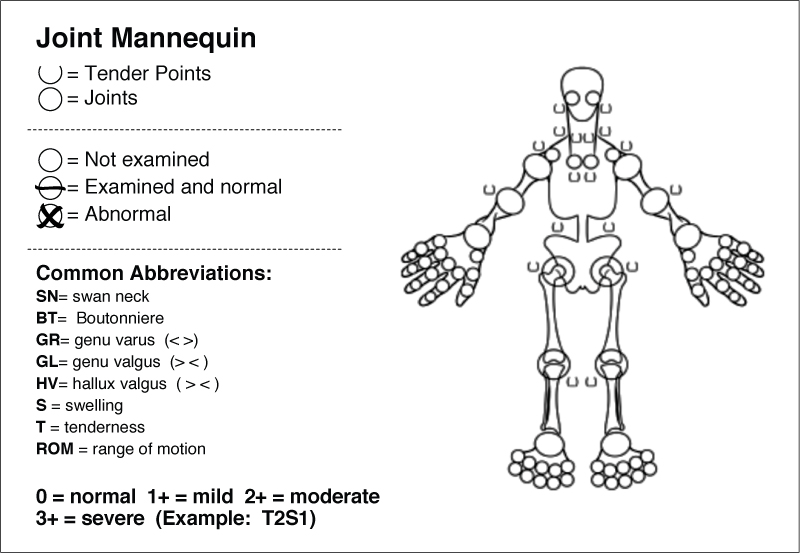
The convention used in musculo-skeletal examination is the "STL" system ( S = swelling, T = tenderness, L = limitation).
Swelling is graded 0 - 3 ( 0 = none, 1 = mild, 2 = moderate and 3 = marked). Swelling may reflect synovial proliferation (pannus) or fluid. Apparent swelling includes bony enlargement and thickening of overlying structures ( skin/subcutaneous fat) or atrophy of surrounding tissues. (skin/muscles especially in the elderly)
Tenderness is also graded 0 - 3 (0= none, 1 = patient says it is tender, 2 = says it is tender and winces, 3 = says it is tender, winces and withdraws). The amount of pressure should be sufficient to cause whitening of the examiner's thumbnail. No lateral movement of the examiner’s thumb should occur during assessment of tenderness. For "deep" joints (shoulders and hips), tenderness is elicited by movement rather than direct palpation.
Limitation of motion is also graded but the range is 0 - 5 ( 0 = full range of motion [ROM], 1 = 1-9% loss of ROM, 2 = 10-19% loss of ROM, 3 = 20-49% loss of ROM, 4 = 50-99% loss of ROM, 5 = ankylosis). Hand ROM can be quickly assessed by recording "fist" formation in percent and grip strength as good/fair/poor. Detailed evaluation of the hand can be requested to occupational therapy (OT).
This general description of the musculo-skeletal examination serves well as a foundation for an adequate general assessment. It can be done in 15 minutes or less. Depending on the initial findings, however, more specific diagnostic tests are required and a more precise measurement of range of motion may be needed. These skills, and knowing when to implement them, can only be gained by practice.
Writing or dictating the musculoskeletal examination
A complete description of the MS examination is vital for demonstrating that a complete examination was performed and to allow the reader to know exactly what was found. It also impacts the billing code. Each area evaluated must be addressed in terms of tenderness, swelling, range of motion and function. Joints, soft tissues (muscles, tender points, tendons and bursas) must be addressed.
Below are examples extracted from patient’s records that show you how colleagues address these requirements:
NORMAL
MUSCULOSKELETAL: Small joints of the hands without erythema, warmth, swelling or tenderness. Good range of motion and function. Wrists, elbows, shoulders without erythema, warmth, swelling or tenderness. Good range of motion and function. Hips, knees ankles, and feet without synovitis or tenderness. Good range of motion and function . Tender points are absent. Percussion of heels not painful and compression of Achilles tendon is not painful. Compression of muscles groups are not tender. SPINE: Examination revealed no gross deformities. No tenderness to percussion. Good range of motion. Schober’s test is __/10/__. Fingertip to floor is ___________cm.
ABNORMAL
MUSCULOSKELETAL: There is bony prominence of the DIP and PIP joints. The MCP joints, wrists are unremarkable without synovitis, have good range of motion and function. Elbows, shoulders with minimal loss of internal rotation in the latter and function and range of motion otherwise preserved. In the lower extremities hips without tenderness, loss of range of motion, have good function. Positive crepitus in the knee but no synovitis, fluid and good range of motion and function. She has the loss of fat pads in both heels. She has marked diminished range of motion of the left ankle with 1+ swelling but no tenderness. Feet with mild “cocking up” of the toes and hallux valgus deformities bilaterally.
SPINE: Examination revealed mild kyphosis. No tenderness to percussion. Good range of motion. Schober’s test is 15/10/9. Fingertip to floor is 6 cm.
The following section has a pictorial outline of the musculo-skeletal examination. Use it to learn the proper manner of examination. Avoid movements beyond those suggested since they tend to be of little help and only give the illusion of thoroughness.